The Patient
Unit 4: Preoperative Assessment & Management
Topic 4: Collecting and Organising Information
Why keep records?
- They form the basis of patient care - where you organize your approach to the patient's problem(s).
- Communication - records should be good enough to permit a colleague previously unfamiliar with the case to take over case with ease.
- Documentation - will you recall signs, test results, drugs and doses without a "hard copy"? Details are soon forgotten, they must be recorded immediately.
- Case records may form the basis of further study and research: incomplete records make such research meaningless.
- Legal evidence - case records form the basis of any investigation of the management of a case: all notes, lab. reports, radiographs, etc. should be kept. The medical record is a confidential document and may not be released to any 3rd party without the consent of the animal's owner.
Recording Systems

There are many diverse record systems used in veterinary practice, from simple cards to complex "problem oriented" folders, to computer-based practice management systems. Small one or two-person clinics often manage with simple card files, while teaching institutions will favour the problem-oriented approach, which encourages students to think!
Many practices now use computer-based recording systems, which largely do away with "hard copy" record storage. These systems offer the advantages of near-instant filing and retrieval and allow many types of manipulations of stored data.
A Good Recording System should include
- Client and Patient identification data
- A "Master Problem" list that summarizes and compiles problems over the patient's life and may also record vaccination and worming data.
- History and Examination records for each visit.
- Progress notes used during periods of hospitalisation.
- Laboratory, radiology and surgical reports.
The Problem-Oriented Veterinary Medical Record (POVMR) System
This system, devised by Dr. Lawrence Weed, organizes patient data and clinicians thoughts into problems in such a way that it assists problem resolution.
There are 4 components of the system:
- Data base: collecting information
- Problem list: deciding what is wrong
- Plans: what to do about each problem
- Progress notes: document and evaluate the chosen plans.
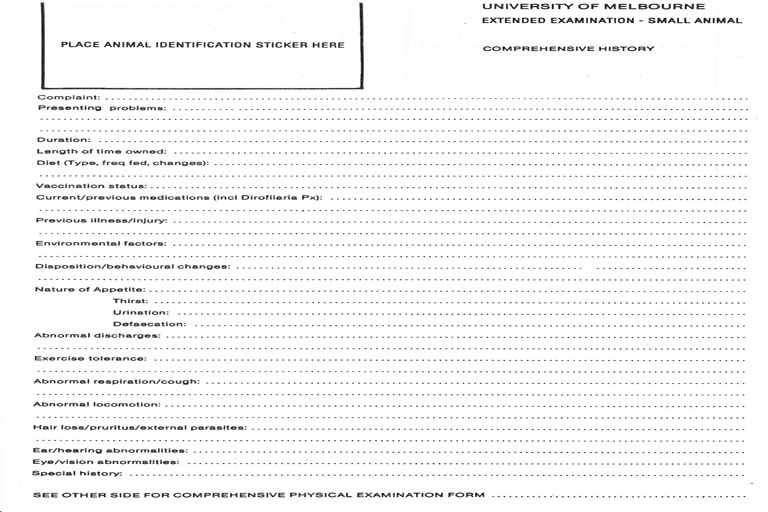
1) Gathering the data base:
Consists of the client's complaints, patient history, results of clinical examination and any available test results
(see Topics 1, 2 & 3). This will be adequate for most simple cases. Complex medical cases may require a more extensive data base, usually directed towards the type of problem.
2) Problem List:
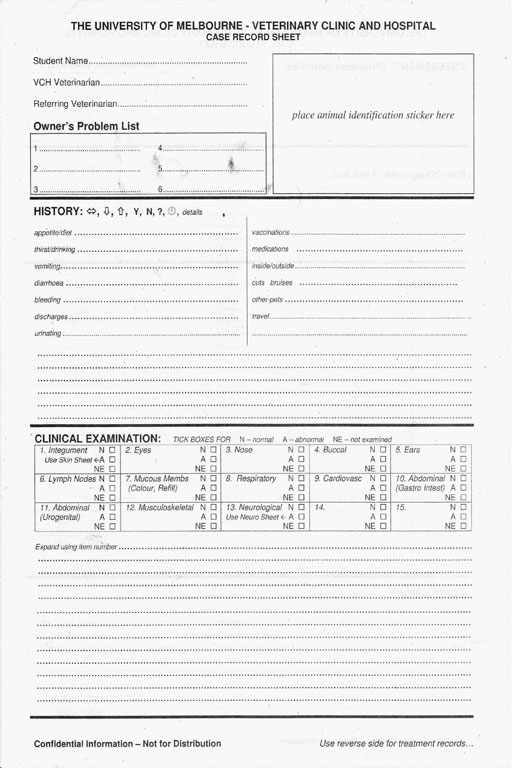
This forms the starting point for action on the case. All problems discovered are listed and numbered. The problem is defined at its current level of understanding.
The Master Problem List forms a listed summary of problems over a patient's lifetime. Problems listed may subsequently be resolved, redefined with better understanding, combined with other problems, or left open.
3) Plans:
These are usually developed on the progress note sheets of hospitalised cases. Each active problem requires a plan for each day. Plans are written using the SOAP format:
S - Subjective information: client history, owner observations, services required by client.
O - Objective data: results of physical exam, lab. tests, radiography etc.
A - Assessment: diagnosis or current understanding of the problem based on subjective and objective data, and prognosis.
P - Plans for management, in 3 categories:
- Diagnostic: what further tests are needed to finalize the diagnosis.
- Treatment: includes drugs, dosages, duration of treatment and goals of treatment.
- Client Education: what the client needs to know about the problem.
SOAP is done at least once each day for each active problem: if new data arrive during the day, the SOAP is rewritten summarizing the updated situation.
SOAP is also written at discharge, summarizing the situation at that time.
Other types of records are used in special situations:
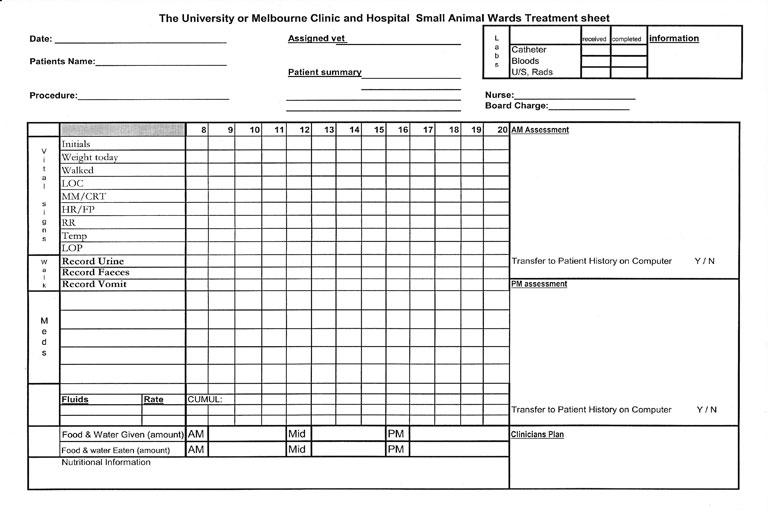
FLOW CHARTS are particularly useful for complex medical cases and to show progression of rapidly-changing clinical parameters: you will see this type of charting used regularly in the emergency/intensive care unit. These charts allow one to quickly get a clear picture of the patient's status and therefore what needs to be done next.
An example of these are the charts used to monitor anaesthetics.