The Patient
Unit 7: Wound Healing and Management
Topic 2: Wound Types
The degree to which the mechanisms of fibrous wound healing occur depends on the type of wound, and the tissues in which they are occurring. In this regard, the wounds may undergo contraction, and if the tissues have an epithelial or endothelial lining, the fibrous scar will become covered with these cells in the process of epithelialization/endothelialization.

Sutured Wound
First Intention Healing
First intention healing occurs in a simple incised or sutured wound. All 4 stages of healing are seen, although the stage of debridement is short and the resultant scar is minimal.
First intention healing depends upon 4 factors:
- Minimal tissue damage
- Minimal dead tissue space
- Minimal contamination
- Wound edges approximated under physiological degrees of tension.
Secondary Intention Healing

Large open wound
Considerations:
- Tissue damage is usually extensive eg. full thickness skin loss
- Considerable dead tissue space may be present
- Contamination is expected
- Wound edges separate
The 4 stages of healing still occur but are more prolonged. The open wound is initially covered by a fibrin clot, then a scab, and then fluid is slowly evaporated from the clot. Within 4-5 days, the wound bed is invaded by fibroblasts and new capillaries are formed. This produces the typical granulating surface (rough, firm and red). Such a surface is very important as it is:

Granulating wound 2
- extremely resistant to infection;
- a surface across which epithelium can migrate;
- contains the mechanism of wound contraction (myofibroblasts) within the granulating surface.
In a full thickness skin wound, the healing process then proceeds by a combination of epithelialization and wound contracture.
Epithelialization
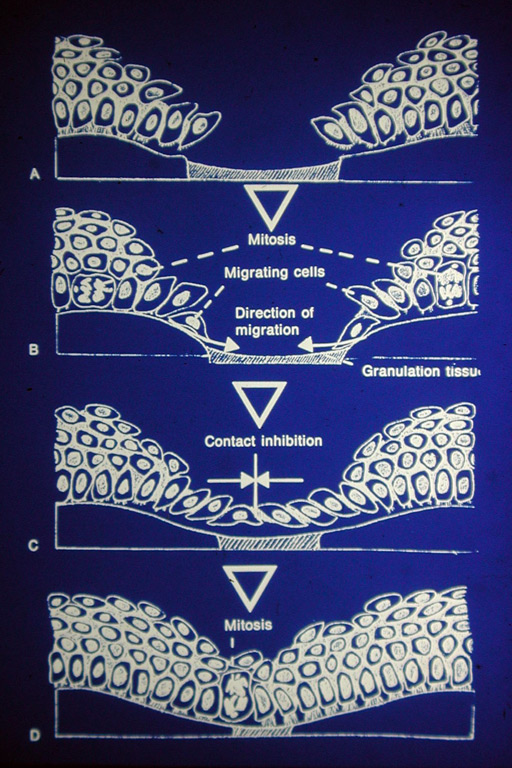
Drawing Epithelial Migration
This starts within 12 hours of injury and may be complete in 12-24 hours in an incised wound.
At the margin of the wound, the epithelium thickens by cell division in the deep skin layers. The epithelium advances across the wound, usually as a single layer of flattened cells across the granulating bed.

Fully Epithelialized wound
Epithelial cells migrate from both the edges of the wound and from remnants of hair follicles (if the wound is not full-thickness). The epithelial cells grow beneath the blood clot by secreting proteolytic enzymes.
Histologically, the migrating epithelium resembles a return to embryonic status with mitosis and pleomorphism, all characteristics of malignant neoplasia. Normal tissue, however, returns to its resting state once healing is complete.
In an open wound, migration is initially rapid but then slows as cells migrate and spread out to a monolayer. Days or weeks may be required to completely epithelialize a large wound. After 4-5 days this is aided by wound contracture.
Cell division and movement begins and continues until the cells are surrounded by other cells of their own type - a process known as contact inhibition.
A tissue hormone known as a chalone is believed to control epithelial cell division and migration. Chalones are water-soluble glycoproteins, located in the epidermis, that have an inhibitory effect on epithelial proliferation. Normally in the non-wounded skin the concentration of chalone is sufficient to suppress mitosis and promote cell function. Damage to the epithelium results in a decrease in the concentration of the chalone and an increase in mitosis. When the cells migrate and meet there is again an increase in the chalone concentration to suppress further mitosis.
Wound Contraction
Wound contraction is an active process centred within the granulation tissue.
Fibroblasts within the granulation tissue develop characteristics similar to smooth muscle. These were called myofibroblasts.
There is a lag period of 5-9 days before a wound starts to contract, which corresponds to the time required for fibroblasts to appear in the wound. Once evident, wound contracture
-3d.jpg)
Horse wounds 1-4
continues until complete and contact inhibition occurs, or contraction ceases due to tension in the surrounding tissues overcoming the force of contracture.
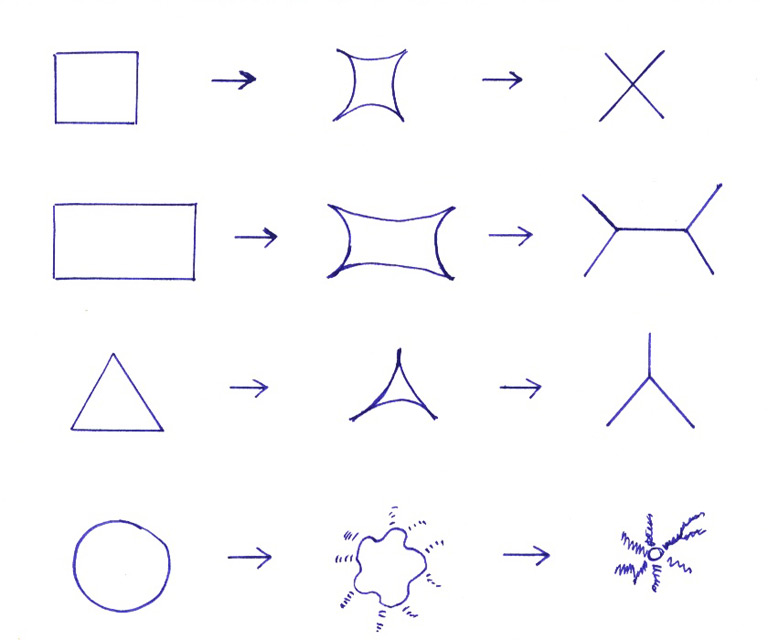
Wound Shapes
The wound shape also has a significant influence on contracture and the final appearance of the scar. Rectangular, square and triangular wounds heal in a star-shape due to contact inhibition at the corners. Circular wounds on the other hand contract in a complicated, unpredictable pattern and are 30% slower to heal with a poor cosmetic appearance.

Contracted wound on thigh
Disadvantages of Contraction
Compared to man, deformity and loss of function due to wound contraction are not a common problem in animals.
Some problems occasionally seen are:
- tight webs of skin over the flexor surface of a joint.
- stenosis of a body opening eg the anus.
Contracture of a wound can be minimised by the use of plastic surgery techniques or full thickness skin grafts. These must be done before contracture starts.