The Patient
Unit 6: Intraoperative Considerations
Topic 4: Haemostasis

Every animal depends upon a properly functioning haemostatic mechanism every day. During surgery, the amount of blood lost will be increased, and a normal haemostatic mechanism is essential in minimizing blood loss.
Haemostasis is important because:
- Excess bleeding obscures the operative field;
- Blood on cloth drapes allows passage of bacteria through the drapes into the surgical field;
- Post-operative haemorrhage or haematoma formation delays healing and encourages infection;
- Protracted haemorrhage may result in anaemia, poor healing or haemorrhagic shock.
Spontaneous arrest of haemorrhage
Three factors are involved in the spontaneous arrest of haemorrhage.
- Extravascular factor
This is associated with the location of the vessel and elastic nature of surrounding tissue resisting the outpouring of blood.
If there is little surrounding tissue or tissue elasticity a haematoma may form. - Vascular factor
Associated with the vessel itself. When a vessel is severed, the intima rolls inwards and the ends of the vessels retract. Exposed collagens in the vessel wall promote platelet aggregation and the formation of a clot. - Intravascular factors
Associated with blood components involved in the clotting mechanisms (Intrinsic and extrinsic pathways). These have been covered in other subjects and should be reviewed for the purpose of this course.
Minimising haemorrhage at surgery
Avoiding, or minimizing the likelihood of haemorrhage, and its effects during a surgical procedure is always preferential to managing haemorrhage once it has occurred.
This can be achieved in a number of ways:
History
A complete including breeding eg. Dobermans (von Willebrand disease), previous bleeding episodes, exposure to drugs eg. aspirin
Physical examination
Conditions which may depress haemostasis or bone marrow activity eg. liver disease, uraemia, should be recognized by laboratory assessment of PCV, TPP, platelets, coagulation profiles (BMBT, Platelet function tests, ACT, APTT).
Preparation for surgery if you suspect excess haemorrhage might occur
Crossmatching of blood, the availability of fresh frozen plasma, cryoprecipitate, and Desmopressin might all be usefully done prior to the surgical procedure.
The use of blunt dissection and surgical technique
Surgical dissection along anatomic planes and minimising incising vessels and muscles are important principles to follow.
Control of Haemorrhage
Surgical trauma will frequently result in damage to blood vessels of the size which cannot be stopped from bleeding by the natural haemostatic mechanisms.
Historically the earliest methods of haemorrhage control were compression and immobilisation. Application of mud, herbs and poultices was also practiced.
Hypocrites used cautery (heat or chemical) in the treatment of haemorrhoids and other diseases associated with bleeding.
Ligatures have been used for over 4000 years. In a comprehensive work, Celsus described the treatment of haemorrhage by the use of pressure, styptics, astringents ligatures and cautery.
Galen in the second century AD recommended silk for sutures.
Current methods used to control haemorrhage:
A large number of methods can be employed by the veterinary surgeon to control haemorrhage. These are listed below and can be considered to be presented in a hierarchical fashion in which the easiest technique is listed first followed by more aggressive techniques which can be employed to larger arteries and veins.
Compression

Digital pressure with the use of gauze swabs is often adequate to control bleeding and slow the flow of blood until the natural haemostatic mechanisms take effect. The pressure may need to be applied continually for 2-3 minutes.

Do not wipe swabs over the tissues to control hemorrhage as this will merely wipe away developing blood clots and prolong haemorrhage.
Compression dressings can also be utilized to minimize haemorrhage.
Crushing
The use of haemostatic forceps on severed blood vessels will stimulate vasoconstriction and clot formation (by the exposure of sub-endothelial collagen, a potent platelet activator), as well as physically preventing bleeding whilst a clot forms.
It is important to use only the tips of the haemostats on the severed vessel to avoid damage to surrounding tissues.
Torsion
Twisting of the blood vessel (with no adjacent tissue) contained in haemostat will create further damage to the vessel wall and exposure of the sub-endothelial collagen to further promote haemostasis.
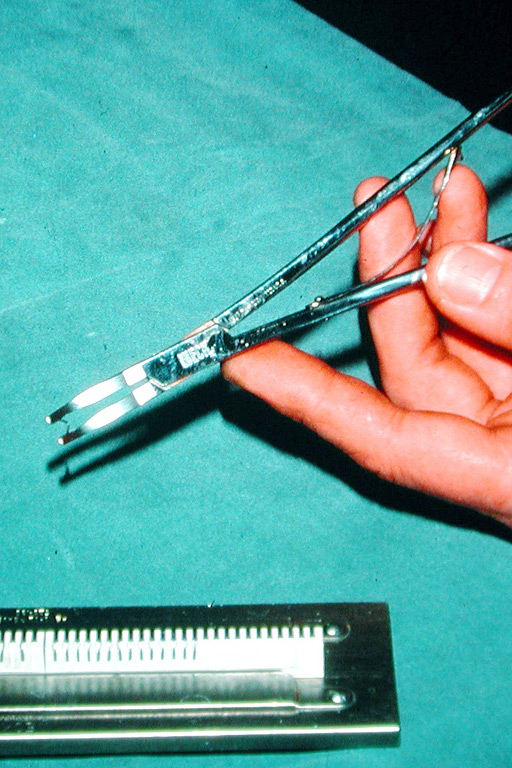
Ligation
Large blood vessels that are identified in the surgical field, or isolated with haemostats can be physically closed with the use of a ligature.
Either absorbable suture materials or non-absorbable materials can be used.
Silk is the traditional material used to ligate large blood vessels.
When ligating a clamped vessel, remove the clamp as the tension is being placed on the thread to allow adequate crushing of the tissues.
An alternative to suture materials is the use of metal ligation clips (Ligaclips - Ethicon, Weck clips).
Transfixing suture ligatures can be used on the uterine stump or as a second ligature on a major vessel to ensure that it does not slip off.

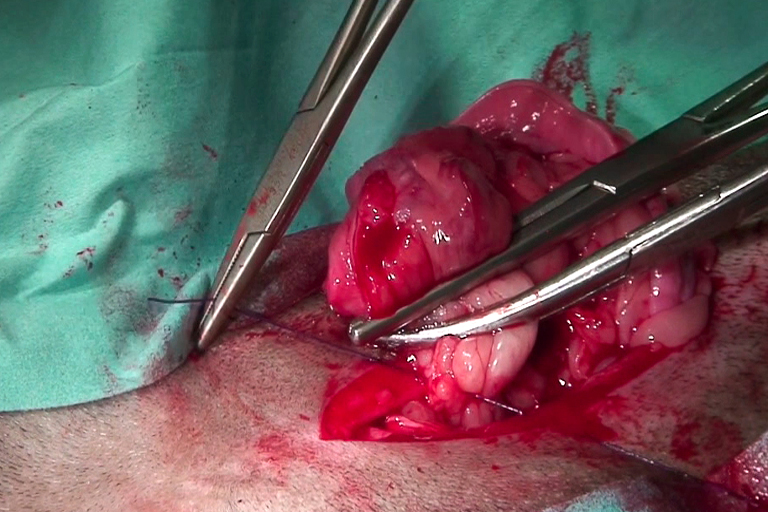
Suturing
Large blood vessels may also be repaired by suturing to maintain their patency. Vascular clamps are applied to temporarily occlude the vessel and allow the repair to be completed. Polypropylene is recognised as the suture of choice for its haemocompatible
characteristics.
Link to Polypropylene sutures
Tourniquets
Tourniquets can be very useful in surgery in reducing the amount of blood loss during a procedure on tissues rich in blood vessels eg. The lower limbs.
They do NOT provide complete or permanent haemostasis but merely slow blood loss.
They should only be applied for short periods of time (less than 3 hours), or significant tissue ischaemia occurs with prolonged use.
An Esmarch's bandage is a type of tourniquet used in the distal limbs of horses.
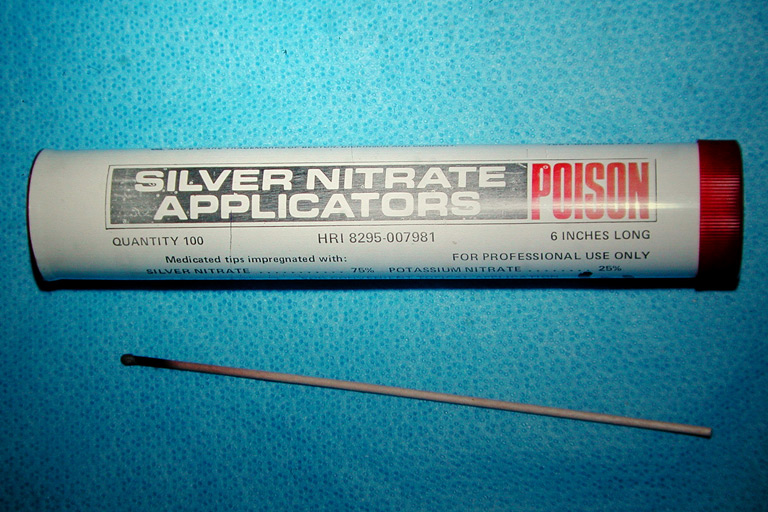
Topical haemostatic agents - Styptics
Topical haemostatic agents can be used to encourage haemostasis in tissues (usually open wounds) with trauma to small blood vessels.
Topical haemostatic agents include:
- Adrenaline, (1mg adrenaline tartrate in 500ml cold saline) used as a lavage results in vasoconstriction and temporary control of haemorrhage.
- ferric chloride
- silver nitrate (useful for bleeding following nail clips)
Absorbable haemostatic agents
Absorbable haemostatic agents are usually composed of a sheet of material or powder composed of an agent which stimulates the clotting mechanism. They are commonly applied to tissues or organs rich in small blood vessels eg. The cut surface of the liver.
A variety of agents are available commercially. They include:
- gelatin sponge (Gelfoam)
- oxidised cellulose (Surgical)
- calcium alginate fibres (Kaltostat)
- fibrin sealants and glues
- topical thrombin
- bone wax
Systemic haemostatic agents
Agents which delay fibrinolytic activity (Tranexamic acid (Vasolamin 10-15mg/kg IM or SC); delta-aminocaproic acid (Amicar)) have been used as systemically administered haemostatic agents with variable effect.
Vitamin K can also be used in cases of warfarin poisoning (Koagulon 0.25-2.5 mg/kg IM or SC).
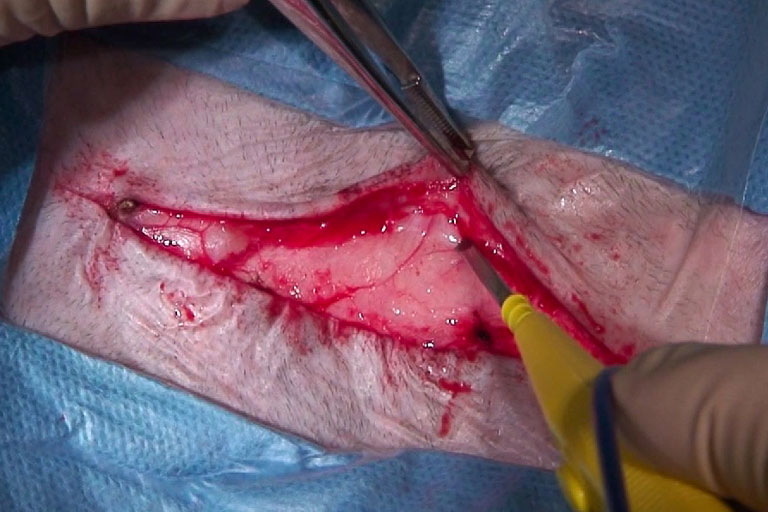
Surgical Diathermy
Surgical diathermy or electro-surgery is the use of energy created by high frequency alternating current traveling between two electrodes to produce local heat in the tissues.
Heat is produced as electric current attempts to travel through the tissues (which act as a resistor) from one electrode to the other. Although the electrodes remain cold, the heat created results in tissue injury and protein coagulation.
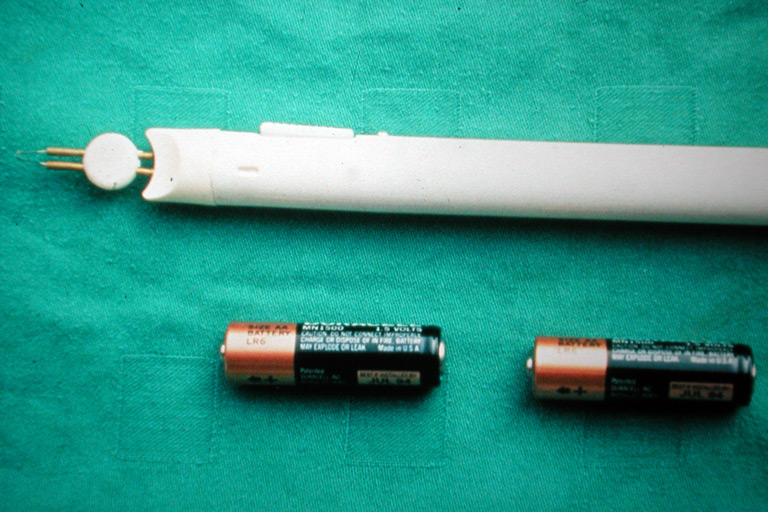
This is to be distinguished from thermocautery which is the direct application of heat to tissues to achieve protein coagulation. Electrocautery uses an electric current to heat a needle or wire to red hot temperatures that cause charring of tissue.

Three types of action can be produced on tissues depending on the characteristics of the current:
- Electrocoagulation, using partially rectified, intermittent current, can seal vessels with diameters up to 1 mm for arteries and 2 mm for veins. If two large electrodes are used, the heat is dispersed over a large area and no injury occurs. Electrocoagulation can however be created if this emitting electrode is reduced to a small tip such as between a bipolar forcep whose arms are the electrodes. The heat produced at the point of contact is sufficient to cause localised tissue injury and coagulation.The heat generated cooks rather than chars tissue, producing white coagulation. The coagulation can be produced by direct contact of the electrode to the vessel (obliterative coagulation) or applying the electrode to an instrument such as a haemostat or tissue forceps occluding the vessel (coaptive coagulation). Electrocoagulation produces white coagulation.
- Electrocutting, using fully rectified, fully filtered continuous current is used to incise tissues by drawing a fine electrode along the tissues. The second electrode is a wide base-plate positioned under the patient so that the current travelling through the body is rapidly dispersed leaving the current which can cause tissue injury concentrated only 1-2mm from the tip of the fine electrode. The incision therefore occurs by internal volatilisation of the cells along the path of the electrode with little damage to the adjacent tissue. Wounds made by electrocutting have lower breaking strength than wounds made by sharp incision for as long as 40 days.
- Fulguration is a high frequency, high Voltage and low Wattage. A spark is generated between the tissue and electrode tip which destroys only the superficial layers of diseased tissues.
Modern equipment uses high frequency currents ranging between 1.5 and 7.5 MHz (optimum cutting frequency is 3.8MHz) and have a power output of around 140 Watts.
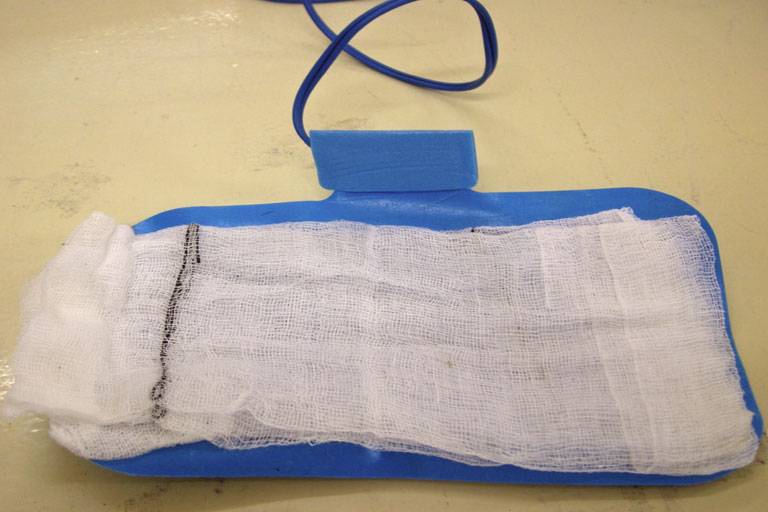
The heat is generated at the tip of a unipolar hand-held electrode with a large plate (electrode) placed under the patient.
Electrosurgery will not work in pools of fluid, and should not be used in the presence of volatile agents (eg. alcohol) or explosive gases. It should not be used near anyone with an unshielded pacemaker!
Electrosurgery will result in slower healing than surgery using scalpel cuts as the body has to undergo a longer debridement phase (see Unit 7) to rid the body of coagulated tissues.
Excessive use of electrocautery has been shown to double infection rates

Fucci, V. & Elkins, AD. (1991) Electrosurgery: principles and guidelines in veterinary medicine. Compend. Contin. Educ. Pract. Vet. 13, 407-415.
Managing the effects of surgical haemorrhage
Prompt management of the patient in which significant haemorrhage has occurred is essential in minimizing the effect of blood loss on the body such as reduced blood pressure and decreased tissue perfusion.
Blood volume replacement will be reviewed in other subjects, but can be achieved with the use of balanced electrolyte solutions, plasma volume expanders or whole blood.
Surgical Haemostasis. J. Niles. In Practice. April 1999, p196-204.